
MEDIA NEWS & RESPONSES TO PUBLISHED ARTICLES
If you have any links to any published news or articles from your local area, and would like to see them published on this page, please email them to us at:
Thank you.
Click on the news article of interest to view:





















Association of Tongue-tie Practitioners-
Responses to published articles:
"Tongue-tie surgery on babies: necessary or needless?"
(The Times, August 2024)
What is it with journalists? Back in January I spoke to Samira Shackle from The Times about tongue-tie division in babies. I kept notes of that conversation. She gave the impression she was going to produce a carefully researched, balanced article on the topic. I think most readers will agree she hasn’t. Certainly, the parents I have spoken to who have read this article were not impressed. The article can be read here.
Unfortunately, despite the rhetoric we get from journalists about objectivity, fairness and impartiality, my experience of late has been that they have set out their position before opening their laptop. When it comes to tongue-tie and infant feeding this is the narrative they all seem to be following:
- Tongue-tie rarely impacts feeding and where it does formula feeding will be the answer.
- Divisions are being carried out unnecessarily and this applies to most divisions being done.
- The majority of babies are not seeing any benefit from the procedure and are suffering complications.
- Parents are being forced to breastfeed and are being misled into thinking breastfeeding offers health advantages over formula feeding.
- The pressure to breastfeed is what is driving parents to seek out tongue-tie division.
They are totally overlooking the fact that breastfeeding is a normal biological reproductive function, just like having the baby in the first place. They are also completely ignoring the fact that the innate desire to breastfeed can be as strong as the longing for a baby. Do we talk about parents being pressured to have babies or scorn those who seek medical treatment when pregnancy doesn’t happen. They are also ignoring the fact that tongue-tie can have a detrimental impact on formula feeding too.
Let’s address the inaccuracies and issues within this article:
According to Shackle ‘anyone’ in the UK can become a tongue-tie practitioner. This is not true. As the NICE Guidance (2005) states, only ‘registered healthcare professionals who are properly trained’ should perform this procedure.
Courses in tongue-tie division are not registered with the Care Quality Commission. Shackle states that they are. All services providing tongue-tie division, whether they provide training or not, have to be registered with the CQC as it is a surgical procedure and therefore a regulated activity under the Health and Social Care Act 2009. Educational programmes are not the remit of the CQC.
As a surgical procedure division has risks like other surgical procedures. It is not accurate to say, ‘There is always a risk of bleeding, infection or damaging healthy tissue if it’s not done properly’. Even when done properly the risks remain. The anatomy influences the level of bleeding as it does in most surgical procedures. There will occasionally be a hidden blood vessel that may get accidentally damaged. We know from the detailed work done on frenulum anatomy by New Zealand ENT surgeon Nikki Mills and her team (Mills, et al, 2019) that some frenula contain muscle fibres. So, these will bleed more when divided.
Infection may occur if an aseptic technique is not observed. But the feeding method will have significant impact on whether an infection occurs or not. Breastfed babies are protected from infections by the anti-microbial properties of breastmilk. Formula, which may be contaminated with bacteria due to incorrect preparation, can cause infection and I have seen this in a baby post tongue-tie division.
Audit data collected by the Association of Tongue-tie Practitioners suggests that less than one in 12000 divisions will result in infection, and around one in 7000 babies will have a significant bleed requiring the topical application of Adrenaline or Tranexamic Acid. In the 7 years ATP has collected incident reports on complications from members there have been no reports of damage to salivary tissue or apnea although these complications are mentioned in the literature. But are clearly rare.
Oral aversion is also rare. In my thirteen years of practice, I have had a handful of babies who have refused to latch after division having latched before division, and I don’t recall any, where the families came back to me for follow up support, who did not re-establish breastfeeding, who have not gone on to latch again. The difficulty is usually short-lived and temporary with the right support.
Shackle suggests there is a lack of research on tongue-tie division. Back in 2005 when the NICE Guidance was written the scientific evidence available at that point was considered adequate by the panel of experts.
Since then, there have been dozens of papers published on this issue. We have six randomised control trials and there have been nine Systematic Reviews with the most recent concluding ‘Results support that infant frenotomy is effective for improving standardised scores on breastfeeding difficulty and maternal pain scales and could improve breastfeeding outcomes.’ (Bruney, et al, 2022)
From these there is clear evidence that tongue-tie division can help improve latch and resolve nipple pain. Four studies on reflux, one focusing on bottle fed babies (Hand, et al. 2023). have concluded that tongue-tie division helps resolve or reduce reflux symptoms in the majority of babies where tongue-tie was present, and these improvements were sustained at 6 months post division. Given the side effects of the unlicensed medications currently being offered to these babies (Lassalle, et al, 2023)and the cost to the NHS of reflux and allergy formulas (which I often see prescribed when the reflux is not allergy related) a thorough feeding assessment as per NICE (2015), including an assessment for tongue-tie, ought to be carried out prior to writing prescriptions.
There have also been studies done using ultrasound and MRI (Watson Genna et al, 2021 and Mills et al, 2020) which have established how a baby uses their tongue during breastfeeding and indeed bottle feeding, and how the function of the tongue is impaired in tongue-tied babies. Elevation, peristalsis, extension and cupping have been identified as the key movements involved in latching to and transferring milk from the breast. Palate shape will also impact, with a high arched palate exacerbating the impact of a restriction in tongue elevation. We have the long established Hazelbaker Assessment Tool for Lingual Frenulum Function which has been evaluated for reliability and validity (Amir et al, 2006) and includes these movements identified in the ultrasound and MRI studies. This tool can help aid assessment and decision making.
Disappointingly, rather than looking at the original research papers and seeking views from academics in the field of lactation and infant/maternal health, Shackle chooses economist Oster’s book ‘Cribsheet’ as her reference source. My friend and colleague Dr Caroline Zwierzchowska-Dod wrote a critique of ‘Cribsheet’ which parents, and indeed journalists, should find helpful to read here.
If you want your work to be taken seriously, I would think looking beyond Amazon reviews, and how many followers someone has on Instagram, when looking at sources of information, would be a good place to start.
Shackle states that the vast majority of divisions take place in the private sector. Given that NHS England cannot provide accurate data on how many divisions the NHS does each year and no one collates data from private practitioners this is speculation. But that is not made clear in the article.
The British study referred to by Shackle is the FROSTTIE study which was presented to the Association of Tongue-tie Practitioners before it was launched. Members at that meeting raised several concerns about the study design which were ignored and that is why it failed. Poor design. It is wholly unfair to lay the blame for the failure of the study on mothers. When the mothers attended the NHS services participating in the study, they had already endured weeks of feeding difficulties and inconsistent feeding support. Who can blame them for opting for an intervention, which the published research confirms can help some babies, rather than allowing themselves to be allocated to a control group for further months of struggle.
It is notable that Shackle doesn’t quote a story from anyone who had a positive, straight forward outcome from a tongue-tie division. Yet, all of us providing tongue-tie division must be CQC registered and as part of that carry out follow-up surveys with our clients so we can demonstrate to the CQC that we are being effective. Virtually all my clients come to me after recommendations from friends and family, or healthcare professionals and breastfeeding supporters, who have experienced or witnessed the positive outcomes that are achieved in the majority of cases. This holds true for many of my colleagues.
Parents are naturally protective of their babies and don’t, in my experience, take the decision to put their babies through a procedure lightly. They do their research. They read, they ask other parents, they talk to healthcare professionals. Shackle would have us believe that parents are blindly pursing tongue-tie division based on having the benefits of breastfeeding ‘drummed’ into them. Well, that ‘drumming’ is failing miserably when you look at the UK breastfeeding rates which Shackle herself quotes as being ‘extremely low’ with 81% of women choosing to initiate breastfeeding and only 12% still exclusively breastfeeding at 4 months. So, isn’t the story here as much about the failure of our healthcare system and society to support these women in their choices, rather than just about babies being put through needless procedures?
Sarianah’s story within the article demonstrates the lack of decent breastfeeding support even in private hospitals which are not under the pressures faced by the NHS. I absolutely acknowledge that there are tongue-tie divisions being done unnecessarily and that a lot of the poor outcomes we see after division are down to a failure to adequately assess, identify and address all the factors contributing to the presenting feeding difficulties. This was something I was at pains to explain to Shackle when I spoke to her.
Shackle goes on to talk about the use of exercises before tongue-tie division or as an alternative to tongue-tie division. Having suggested there is ‘inconclusive’ evidence of tongue-tie division being helpful in addressing feeding difficulties, despite the published papers on this, she overlooks the fact there is currently no published evidence to support the exercises approach. I have seen families where practitioners have suggested they follow a regimen of exercises for weeks, or in some cases months, before a division or as an alternative to division and there has been no improvement in feeding. In fact, in most of the cases that have come to me, feeding has deteriorated with mothers moving from fully breastfeeding to combination feeding or formula feeding before finally coming to me for a division. Upon assessment these babies have still had significant restriction in their tongue function. I have colleagues who have had the same experience. Whilst a lot of us advocate exercises post division, and there may be some value in starting these pre division, I am not aware of a single piece of published research suggesting there are any specific exercises that are an effective alternative to tongue-tie division where tongue function is significantly compromised by a tight lingual frenulum and impacting feeding.
I think many breastfeeding mothers who have experienced excruciating nipple pain and seen their babies lose weight because of a tongue-tie would disagree with the assertion that tongue-tie division ‘is not an emergency procedure’ and the suggestion that we can spend weeks on unproven exercises. In some cases, where a tongue-tie is causing severe difficulty with establishing breastfeeding, early intervention with a tongue-tie division will be crucial in helping mothers sustain breastfeeding. David Todd (2015) a neonatologist in Australia published audit data which confirmed the negative impact on breastfeeding duration when division is delayed and not offered in acute cases in the first few days of life.
What many practitioners and families do report as useful is body work (cranial osteopathy, cranial sacral therapy and chiropractic). I avoid a significant number of divisions be referring to body work first, alongside feeding management strategies, and see significant improvements when this therapy is combined with tongue-tie divisions in cases where the baby has muscular and fascial tensions related to in utero positioning and the process of birth. We have a growing body of published research on the role of bodywork in addressing infant feeding difficulties. Yet, Shackle doesn’t mention this at all.
We need to be asking questions about the apparent rise in the numbers of babies being diagnosed and treated for tongue-tie. We need to ask questions about why parents are being offered frenulotomy in babies for issues other than feeding when there is no evidence to support this. We need to be looking at how babies are being assessed and how families are being supported with feeding prior to being offered divisions. We also need to be ensuring there is skilled support offered to them afterwards. We certainly need to be looking beyond the lingual frenulum and frenulotomy for answers to feeding difficulties. We absolutely should not be questioning the desire pf mothers to breastfeed or whether breastfeeding is beneficial to babies. The research on that is clear and not up for debate. We should be demanding better care and support for all families. However, they choose to feed their babies because both breastfeeding and formula feeding can present parents with huge challenges and families continue to be failed and deserve better.
As for journalists they need to set their own experiences and prejudice aside and open their minds. I am horrified that the editor of The Sunday Times allowed such a biased article to be published. What else is The Times misleading us all on? Within this article there are very valid points and issues raised that warrant further exploration, but this journalist’s preset agenda has got in the way of that.
Sarah Oakley BA (Hons) RN IBCLC
14/08/2024
Rapid Response:
"Posterior tongue-tie and lip tie: a lucrative private industry where the evidence is uncertain."
(February 2021)
doi https://doi.org/10.1136/bmj.m3928 British Medical Journal 2020;371:m3928
In reference to the article entitled:
“Posterior tongue-tie and lip tie: a lucrative private industry where the evidence is uncertain” published 26th November 2020 as an abridged version of an earlier article published in the BMJ Opinion on 2nd October 2020.
Dear Editor,
The Association of Tongue-tie Practitioners (ATP) is a UK organisation which was set up in 2012 by a group of tongue-tie practitioners from the NHS and independent sectors. We aim to promote the awareness of tongue-tie as an infant feeding issue, providing educational opportunities for healthcare professionals and infant feeding supporters. We provide support and opportunities to share best practice for those dividing tongue-ties working both independently and within the NHS. We provide information for parents and facilitate them to access safe and effective care regarding tongue-tie. We read the article mentioned above and would like to make some comments.
The article states that division of a tongue-tie is carried out “usually in an ENT outpatient setting”. We would disagree, as the majority of divisions are performed outside of the ENT setting. Examples would be children outpatient departments, hospital wards, private and NHS community clinic settings, dental surgeries and in private homes.
Despite many audits and parental feedback surveys carried out by our members confirming the positive impact of tongue-tie division, we do agree with the need for further randomised controlled trials of high methodological quality.
Many of our practitioners are now reluctant to use the term posterior tongue-tie; favouring terms such as ‘restrictive or non-restrictive frenulum’ but may use it to describe a frenulum that is visible but inserts behind the sub mandibular gland openings. The article states “the concept is generally thought to represent a tight – non-visible submucosal band of tissue at the very base of the ventral tongue that is palpated rather than seen”. Many tongue-tie practitioners would question this definition now in light of new work by Mills et al 2019 (1) which is not even referenced by the authors and most relevant to the discussion. This anatomical research has helped us understand the structure of the frenulum and goes as far as to say that the term posterior tongue-tie should not be used.
We do acknowledge that many babies are misdiagnosed with tongue-tie when in fact they have other fascial tensions that could be resolved with physical therapies and skilled feeding assessment and support. Taking a detailed birth and feeding history and using a validated tongue-tie assessment tool such as the Hazelbaker Assessment Tool for Lingual Frenulum Function (2) (3) will help identify whether tongue-tie division might be indicated. Not all breastfeeding support workers are trained to assess for tongue-tie so undoubtably there may be some referrals whereby tongue-tie is suspected but not actually present on full assessment.
The article states “posterior tongue tie is generally not recognised or treated currently by professionals within the NHS setting”. We have many NHS tongue-tie practitioners in our association who would disagree with this assumption. We would have expected the authors to have produced an audit of all NHS practitioners before generalising in this way. It is worth noting that all private practitioners will have been trained to divide all types of tongue-ties within the NHS setting before working in private practice.
Lip tie division is very rarely carried out in this country, and most of our members are of the opinion that lip tie does not affect feeding. Most are of the opinion that lip tie division should only be considered if orthodontics work is required in the older child. We are only aware of a couple of dentists who divide lip ties and ATP have issued a statement on lip tie (4) as we do not believe there is sufficient evidence for lip tie division to help breastfeeding at present.
The article states “usually for a fee of several hundreds of pounds”. This is a very general statement and whilst the authors may well be able to identify certain practitioners who do charge such large fees, many do not. Most private practitioners earn a modest wage which covers the procedure, the skilled assessment and feeding support. Many include ongoing support and advice as part of their charges and have been a great source of help to parents where breastfeeding and tongue-tie services have been more limited within the NHS, especially during the pandemic.
The article states “a quick online search uncovers scores of private practitioners willing to travel to assess and treat newborns for posterior tongue tie….” Practitioners will travel to provide a service, yes, but they are health professionals, working within their professional regulatory body’s code of practice and regulated by the CQC. There is no evidence that any private practitioner specifically mentions or markets themselves as dividing posterior tongue-ties. Most are of the opinion that it is either a tongue-tie or not and that will be determined by skilful assessment. Tongue-tie division will normally only be carried out with the fully informed consent of parents, having explored all other options.
Chair ( Luci Lishman IBCLC RGN RM) representing the committee of the Association of Tongue-tie Practitioners.
References
1. Mills, N., Keough, N., Geddes, D., Pransky, M., Mirjalili, S.A., (2019) Defining the anatomy of the neonatal lingual frenulum. Clinical Anatomy 2019 https://doi.org/10.1002/ca.23410
2. Amir, L.H., James,J.P.,Donath, S.M. (2006) Reliability of the Hazelbaker Assessment Tool For Lingual Frenulum Function. International Breastfeeding Journal 2006
3. Hazelbaker, A.K (2010) Tongue-tie: morphogenesis, impact, assessment and treatment. Aiden and Eva press.
4. Association of Tongue-tie Practitioner’s website ATP Statement on lip tie – 2014
https://www.tongue-tie.org.uk/atp-statement-on-lip-tie/
Competing interests: I work as a private Tongue-tie Practitioner
16 February 2021
L E L Lishman
Tongue-tie Practitioner RM RGN IBCLC
Chair of the Association of Tongue-tie Practitioners
"Does Post-operative Wound Massage Improve Outcome of Frenulotomy for Breastfeeding Difficulties in Infants?"
(November 2014)
Does Postoperative Wound Massage Improve Outcome of Frenulotomy for Breastfeeding Difficulties in Infants? Slothouber Galbreath et al, JHL, Volume 30, Number 4, page 501, November 2014
Dear Editor Re: Does Postoperative Wound Massage Improve Outcome of Frenulotomy for Breastfeeding Difficulties in Infants? Slothouber Galbreath et al, JHL, Volume 30, Number 4, page 501, November 2014.
The Association of Tongue-tie Practitioners is a UK organisation which was set up in 2012 to promote the awareness of tongue-tie as a feeding issue, provide educational opportunities for healthcare professionals and lactation supporters, provide support and opportunities to share best practice for those dividing tongue-ties and provide information for parents. We currently have 97 members. We read the abstract mentioned above with interest and would like to raise some issues which we have set out below.
The Abstract by Slobothouber Galbraith, Fisher and Patel (which we understand was presented at the ILCA Conference 2014 and then printed in the JHL) relates to a study which aimed to assess the compliance, tolerance and efficacy (prevention of recurrence) of disruptive wound management (DWM) following tongue-tie division.
To our knowledge, there are no published controlled trials on DVM. But wound massage and/or stretching following tongue-tie division is advocated by some practitioners including dentist Larry Kotlow (http://kiddsteeth.com/dental_topics.html#breastfeeding_health). But actively disrupting the “wound adhesions in situ” seems to be a step further.
The abstract refers to the methodology as a ‘single operator study’. Members of the Association of Tongue-tie Practitioners attended the 2013 Tongue-tie Symposium held at King’s College Hospital, Croydon where the authors of this abstract did a presentation on this study. It is our understanding that Katherine Fisher (one of the aforementioned authors) was the ‘single operator’ and that no-one else was directly involved in the assessment, treatment and follow up of the breastfeeding dyads. Ms Fisher is a committed believer in DWM and actively trains and firmly encourages all parents to perform it post division. (See Tongue-tie Guide at http://katherinefisher.co.uk/videos-and-downloads/) Hence you would not expect the parents to admit to her or any researcher connected to her that they did not comply. An independent researcher is essential. Of the original 126 dyads, 47 did not reply, and a further 19 responses were “unsuitable”. We would be interested to know why only 60/126 (48%) of parents replied fully?
The results section of the abstract talks about ‘tolerance’. But tolerance is not assessable. Of the 60 “suitable” replies, two thirds (40/60) said that the DWM was tolerable, suggesting that the other third found it intolerable. This group is in addition to the non-responders who may also have found it intolerable. To ask parents to perform an intolerable procedure for no proven gain is ethically difficult and many tongue-tie dividers find impossible to support.
Efficacy is measured by the lack of recurrence and breastfeeding rate. Most tongue-tie dividers accept that there may be a small (<3%) recurrence rate for anterior tongue-ties, not all of whom are symptomatic. For there to be no recurrences in 60 is therefore to be expected and is not evidence for any increased efficacy.
The breastfeeding rate of 92% at 6 weeks is very good, but includes the third who found the DWM intolerable. We do not know if this is 100% breastfeeding, which would be spectacularly good, or just one feed a day. What happened to the ones who did not reply? The actual proven breastfeeding rate is 55/126 (43%), not 92%. A breastfeeding rate at 3 months for all 126 would have been much more useful.
Members of the Association of Tongue-tie Practitioners have received reports of mothers who have been trained to do DWM who were traumatised, whose babies’ tongue-ties have recurred and who then feel to blame for failing to perform the DWM correctly. This is unsatisfactory. The subject of Disruptive Wound Management is so divisive that it is critical that any study published is scientifically useful, so that we can assess if the procedure is one which we should teach our parents. This abstract confirms the views of those who do not think that the trauma of DWM has any use in anterior tongue-ties and has yet to be proven in posterior tongue-ties, whose recurrence rate is higher.
To allow equipoise in a randomised controlled trial of DWM against a control group, you need to be able to show that the intervention group (DWM) is no worse than the control group, has no side-effects which would deter participants and might have a better outcome. From this abstract it is not clear that this study is able to provide this evidence.
Yours faithfully
Suzanne Barber RM IBCLC and Sarah Oakley BA (Hons) RN RHV IBCLC
On behalf of the Committee of the Association of Tongue-tie Practitioners
"Breastfeeding: Mothers are repeatedly told breast is best – but what about the lack of support when babies have tongue-tie?"
The Independent (March 2015)
Dear Editor
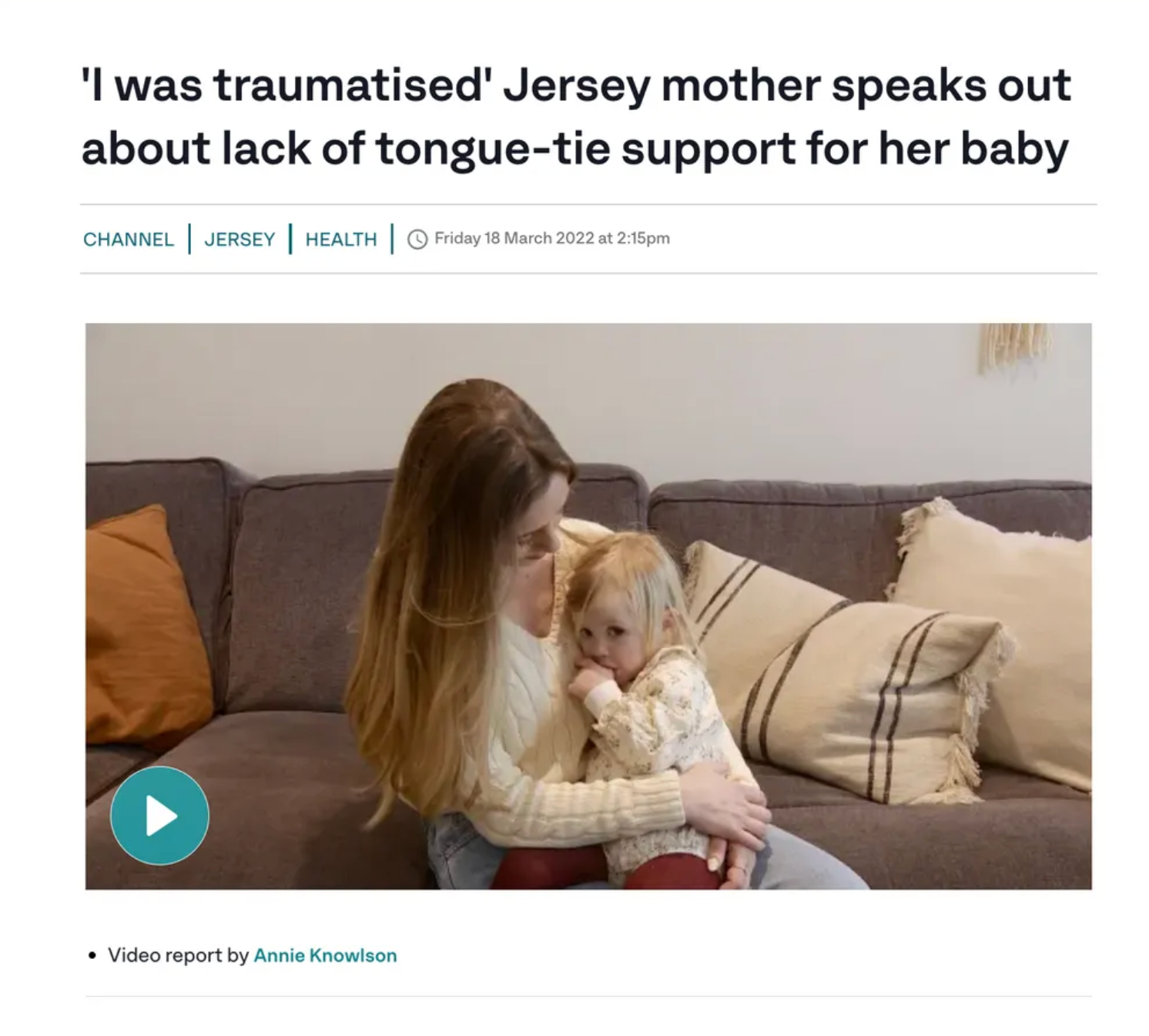
The Association of Tongue-tie Practitioners was delighted to see your report Breastfeeding: Mothers are repeatedly told breast is best – but what about the lack of support when babies have tongue-tie? Wed 18 March edition of The Independent highlighting the issues faced by parents with tongue-tied babies. We were very happy to see that there was a positive outcome for Kate, the mother featured in the case study. Her experience highlights the serious feeding issues that can result from a tongue-tie and the difficulty mothers often face in getting the problem recognised and treated. It is a story that is very familiar to those of us working in breastfeeding support.
Unfortunately for Kate and her son the tongue-tie reoccurred after the first procedure so a second procedure was carried out. Recurrence is a recognised complication of tongue-tie division. But it is believed to affect only a very small percentage of babies. The case study suggests that the thing that led to a positive outcome, after the second division, was the 6 weeks of wound management they followed which Kate refers to as ‘the Kings College Treatment’.
This kind of disruptive wound management (which involves massaging the wound repeatedly over a period of time following tongue tie division) has been promoted by practitioners, not just at Kings College Hospital, but in other parts of the world, particularly in the United States. However, there are some concerns about this approach. Despite the fact that this kind of wound management has been recommended for several years there have been no published controlled studies done to establish its safety or efficacy. There is no agreed consensus on what post procedure wound management should involve. In the case study twice daily for 6 weeks was recommended. Others recommending this approach suggest massaging at every feed for at least a month, whilst some say twice a day for 5 days is sufficient. So it is a confusing situation for practitioners, as well as parents.
In the case study baby Ethan is reported to have tolerated the massage. But there are lots of reports from parents which describe the process as distressing, difficult and traumatic. It can also cause the wound to bleed, which can be frightening for parents, and many parents feel that it is painful for their baby and do not continue with it. There are professional concerns about increased risk of oral aversion and infection. There have also been lots of reports of babies continuing to suffer repeated recurrence of the tongue tie, despite following these massage regimens.
Recurrence of tongue tie is an issue that most definitely needs further research. It still not fully understood why it recurs in some babies and not others, although there are plenty of theories. It remains our experience that most babies do well after tongue tie division without the need for further surgery. A recent informal audit from ATP members found that around 3% of babies were returning for second divisions.
Whilst we fully respect and understand the fact that some parents may feel they would like to follow something like the Kings College Treatment after their baby’s tongue tie is divided, many practitioners feel that until robust research is undertaken it is important that parents understand that, whilst some may believe these approaches are helpful, there is a some way to go before there is a consensus on how best to manage the issue of recurrence of tongue-tie. The importance of skilled breastfeeding support in achieving successful outcomes for mothers and babies should not be underestimated.
Parents and professionals can find more information about tongue-tie at www.tongue-tie.org.uk.
Yours faithfully
Suzanne Barber RM IBCLC and Lynn Timms RHV IBCLC
On behalf of the Association of Tongue-tie Practitioners
"Position statement on the Mum and Baby Academy CPD Module on tongue-tie distributed by various midwifery and nursing journals."
(October 2017)
Position statement on the Mum and Baby Academy CPD Module on tongue-tie distributed by various midwifery and nursing journals in October 2017
The Association of Tongue-tie Practitioners welcomes any opportunity for healthcare professionals to access free learning such as that Mum and Baby Academy offer. However we have reviewed the tongue-tie module after concerns were raised by some of the ATP membership.
In the module the learning objectives are stated as being:
- Be able to identify and assess ankyloglossia in infants
- Understand how ankyloglossia can affect breastfeeding
- Appreciate the ways in which women can be supported to successfully breastfeed babies with ankyloglossia
- Be able to advise and reassure parents about ankyloglossia and frenotomy using evidence-based knowledge.
However, it is the opinion of the ATP committee that the module:
- Fails to adequately describe how tongue-tie is classified or assessed and provides irrelevant information on ‘superior’ tongue-tie which is an entirely different anomaly to a restricted lingual frenulum. Assessment of tongue-tie is complex and practitioners require advanced lactation skills as well as practical experience in examining the mouths of infants, something a short distance learning module cannot provide.
- Fails to explain in any depth how tongue-tie may impact on feeding and doesn’t provide any guidance on strategies that can be used to support mother’s with the various feeding challenges tongue-tie may present.
- Provides confusing and misleading information on how a baby latches to the breast and the role of the lips.
- Gives inadequate information on how tongue-tie division is performed, normal wound healing and complications.
We believe that the learning objectives simply are not met and some of the information provided is inaccurate, irrelevant or incomplete.
As such the ATP does not feel that this module is of sufficiently good quality to meet the learning needs of healthcare professionals supporting mothers and babies with feeding issues associated with tongue-tie. We are also concerned by the sponsorship of the module by Lansinoh, who are not WHO Code complaint, and the accompanying advertisement for their nipple shields, when nipple shield can seriously impair milk transfer in tongue-tied babies.
We suggest that healthcare professionals seek education on this issue from other sources.
Sarah Oakley BA (Hons) RN IBCLC, ATP Chair
"Does Frenulotomy help infants with tongue-tie overcome breastfeeding difficulties?"
(April 2015)
Journal of Family Practice 2015 February;64 (2):126-127. 7 April 2015
Dear Editor
We are writing on behalf of the Association of Tongue-tie Practitioners (www.tongue-tie.org.uk) and Tongue-tie UK, a grass roots organisation which aims to raise awareness of tongue-tie issues (www.tonguetieuk.org) in response to the article by J. Cawse-Lucas et al (2015) Does Frenulotomy help infants with tongue-tie overcome breastfeeding difficulties? Journal of Family Practice 2015 February;64 (2):126-127.
The article begins by answering the question with ‘probably not’ and says that ‘evidence concerning improvements in maternal comfort is conflicting. At best, Frenulotomy improves maternal nipple pain by 10% and maternal subjective sense of improvement over the short term (0 to 2weeks)’.
Research on the efficacy of tongue-tie division is limited. But the article seems to focus only on the RCTs, ignoring other research, and we have some concerns in the way the evidence from these has been interpreted in this article.
The first study cited by Cawse-Lucas J et al (2015) was conducted by Buryk M, Bloom D, Shope T (2011). This was a single blinded RCT involving 58 infants with a mean age of 6 days. The Short-Form McGill Pain Questionnaire (SFMPQ) was used to assess maternal nipple pain before and after Frenulotomy. Mean scores were 16.8 in the intervention group and 19.2 in the control (sham) group prior to Frenulotomy. Immediately after Frenulotomy mean pain scores fell to around 4.5 in the intervention group. There was also some improvement in the control group with scores of 14.5. So some improvement resulting in a mean 4.7 point drop in pain scores was seen without Frenulotomy. However, with Frenulotomy mean pain scores dropped considerably more by 12.3 points. In the intervention group pain scores then fell to about 2.5 at two weeks, one at 4 weeks and to around zero at 2 , 6 and 12 months. All except one participant in the control (sham) group went on to have Frenulotomy by 2 weeks and their pain scores post intervention then showed a similar pattern. So, we are not sure how the conclusion that improvement in pain in this study persisted at two weeks, but not at 4 weeks and beyond has been drawn. The graph in figure one of the Buryk, et al (2011) paper suggests that the nipple pain resolved by around 2 months and remained resolved as pain scores did not then increase.
Cawse-Lucas J et al (2015) then go on to discuss the unblended RCT by Hogan M, Griffiths M, Westcott C (2005). This involved 40 infants, mean age 14 days. Maternal subjective ratings of improvement were gathered by phone interview at 24 hours. Obviously this study does not provide any evidence of long term improvement in feeding. But this is because long term outcomes were not evaluated as part of this study.
Two newer RCTs by Emond A et al (2014) and Berry J, Griffiths D, Westcott C (2012) are then reviewed. J Cawse-Lucas et al (2015) conclude that the former study ‘found no breastfeeding improvements’. Yet the discussion section of the Emond et al (2014) paper states ‘while the simple VAS used in the Bristol Trial (this study) was not sensitive enough to show differences between the groups, the relief of painful sucking provided by Frenulotomy was a clear theme emerging from the qualitative interviews’. The study concluded that early Frenulotomy does improve maternal self efficacy which has been shown to impact positively on breastfeeding duration. It also found that at 5 days a 15.5% increase in bottle feeding in the control group and a 7.5% in the intervention group. So there was some evidence of improvement in pain, albeit subjective and fewer of the intervention group were bottle feeding at 5 days.
The Berry J, et al study, although published in 2012, was in fact conducted in 2003/4. Cawse- Lucas J, et al (2015) state that it found no improvement in breastfeeding. Yet the breastfeeding rate amongst the babies who have received Frenulotomy at the 3 month follow up (mean age 4.5 months) was 50%, almost twice the national average of 29%. It is not unreasonable to assume that Frenulotomy played a part in this impressive figure. Surely the continuation of breastfeeding is the most important measure of success in any breastfeeding intervention.
It is interesting that Cawse-Lucas J et al (2015) refer to the position statement from the Community Paediatrics Committee of the Canadian Paediatric Society (Rowan-Legg A, 2011). However, the authors make no reference to the NICE Guidance (2005) from the UK which concluded that:
Current evidence suggests that there are no major safety concerns about division of ankyloglossia (tongue-tie) and limited evidence suggests that this procedure can improve breastfeeding. This evidence is adequate to support the use of the procedure provided that normal arrangements are in place for consent, audit and clinical governance.
http://www.nice.org.uk/guidance/ipg149/chapter/1-guidance
Furthermore the Canadian position statement (Rowan-Legg A, 2011) is itself contradictory:
Based on current available evidence, Frenulotomy cannot be recommended. If, however, the association between significant tongue-tie and major breastfeeding problems is clearly identified and surgical intervention is deemed necessary, Frenulotomy should be performed by a clinician experienced with the procedure and with appropriate analgesia.
The authors make no reference to the systematic reviews that have found an association between Frenulotomy and improved breastfeeding including Finnigan V & Long T (2013) which looked at 5 RCTS and 9 case studies and concluded that Frenulotomy offers long term improvements in over 50% of cases, Edmunds J, et al (2011) which looked at 25 papers and concluded that ‘frenotomy offered the best chance of improved and continued breastfeeding’ and Ito Y (2014) which concluded that there is an ‘overall moderate quality of evidence for the effectiveness of Frenulotomy for the treatment of breastfeeding difficulties’.
But setting aside the RCTs and systematic reviews, what about the views of mothers. These are some of the comments sent in to Tongue-tie UK by mothers after they read the Cawse-Lucas J et al (2015) article:
‘Made a big difference to us in breastfeeding and our baby was older than the ones studied here. Frankly if it helps with nipple pain then that’s a win as most quit due to pain…Our baby went from the 10th percentile to the 60th 3 months after procedure’.
‘The improvement in every area was unbelievable. My son put on weight and started to thrive and his colic stopped. I’m still feeding him myself now – he turned 15 months today.’
‘We noticed a mild posterior tongue tie in my son at birth but decided not to snip initially as it was so minor. 9 weeks of poor weight gain later and it was really the only thing left to rule out, so we snipped it and he began gaining a pound a week from then on.’
‘My 11 week old son had a severe tongue tie, I was advised to use nipple shields until his tongue tie could be snipped which despite an urgent referral being sent could take a few weeks, despite using shields feeding was excruciating, my nipples were bleeding and I was using tonnes of lanolin… He had his tongue tie snipped at our local hospital when he was 5 days old, I fed him straight after and I noticed an improvement in latch immediately and within days I was able to feed him without the use of nipple shields. Now he feeds beautifully and is gaining weight brilliantly (not that weight was an issue) and I barely even notice he is feeding. I don’t think I would have been able to carry on breastfeeding if he hadn’t had his tongue tie snipped as I was starting to dread feeds and was in seriously excruciating toe curling pain each feed and was so close to giving up.’
‘Straight away feeding was easier, her latch was deeper but I did have to re teach her to feed. It took a good few weeks for the pain to go but neatly 12 months in and we are still feeding.’
There is no doubt that more research is needed in the area of Frenulotomy. But randomised controlled trials are not the only form of evidence we should be considering when looking at outcomes. The very nature of the procedure and breastfeeding difficulties means that RCTS are always going to be fraught with difficulty as it is virtually impossible to blind mothers to the intervention (especially now there is so much information about the procedure, bleeding afterwards and wound healing in the public domain) and there are ethical issues in withholding treatment from the control group which may increase the duration of breastfeeding. Measurement of outcomes is always going to be at least partially subjective as mothers will vary in their expectations and perceptions of breastfeeding.
Qualitative data from mothers needs to be used to inform quantitative research and we need to be cautious about the interpretation of any results. No one is claiming that Frenulotomy is effective at sustaining breastfeeding in all cases. The breastfeeding relationship between a mother and baby is a complex one and for all mothers and babies there will be other factors, other than tongue-tie and Frenulotomy, that influence outcomes. But given the numbers of mothers who give up breastfeeding in the first two weeks and the very low breastfeeding rates we have in most of the Western world we need to explore and offer any interventions,that are deemed safe, which have the potential to help improve breastfeeding duration.
Whilst we are sure the authors of this article did not intend for their medical colleagues to read it and dismiss Frenulotomy as ineffective at improving breastfeeding outcomes, there is a risk that this is how it will be interpreted by many of those who are not working with mothers of tongue-tied babies and are not hearing their stories.
Yours faithfully
Sarah Oakley BA (Hons) RN RHV IBCLC, Deputy Chair Association of Tongue-tie Practitioners
References in addition to those cited in the original article:
Edmunds J, Miles S, Fulbrook P (2011) Tongue-tie and breastfeeding: A review of the literature. Breastfeeding Review 2011:19(1):19-26
Finnigan V, Long T (2013) The effectiveness of frenulotomy on infant feeding outcomes: a systematic review. Evidence Based Midwifery June 2013
Ito Y (2014) Does frenotomy improve breast-feeding difficulties in infants with ankyloglossia? Pediatrics International, 56: 497-505.
Division of Ankyloglossia(tongue-tie) for breastfeeding (2005). NICE Interventional Procedure Guidance (IPG 149)
"Why Folic Acid is not to blame"
There is lots of speculation about a connection between folic acid, the MTHFR gene mutation and the increase in infant tongue-tie incidence. This topic comes up frequently in online parenting groups and sometimes in the wider media. The MTHFR gene provides instructions for making an enzyme called methylenetetrahydrofolate reductase. This enzyme is involved in a chemical reaction involving folate. The theory is that a mutation in this gene leads to folate deficiency and people with this mutation cannot process the folic acid recommended preconception and during pregnancy. Folic acid supplementation is recommended to prevent neural tube defects, such as spina bifida. To date there are no published research papers demonstrating a link between folic acid supplementation and tongue-tie. In fact a study by Perez-Aguirre et al (2018) which looked at folic acid consumption and a number of oral findings in new-borns found no link with tongue-tie.
The evidence suggests that tongue-tie is genetic in origin as it seems to run in families and there may be environmental triggers, as yet unknown. It is imperative that the Department of Health guidelines on folic acid supplementation pre conception and in pregnancy are followed by parents and reinforced by healthcare professionals as this has been shown to be very effective in reducing cases of neural tube defects.

